

Surgical Treatment for Endometriosis
The severity of the disease, the woman's history of infertility, the intensity of her desire for pregnancy, and her age all play a role in determining whether or not to do conservative surgery to restore reproductive structures or to perform a hysterectomy. Unfortunately, even hysterectomy is not a guaranteed cure for the disease as up to 30% of women have persistent pain.
In women with distorted tubal-ovarian anatomy due to endometriosis, the first surgery is the most effective. Repeat surgical interventions are less effective at restoring fertility, than the initial attempt, which is best performed by a skilled endoscopist.
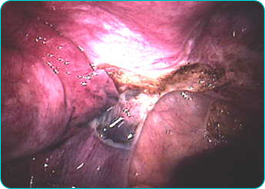
The most common surgical procedures performed with the laparoscope are the cutting and removal (lysis) of pelvic adhesions surrounding the ovaries, tubes, and uterus, excision or surgical removal of endometriotic implants and removal of ovarian endometriomas.
Surgical treatment of endometriosis consists of cautery, coagulation, excision or vaporization. As most cul-de-sac endometriosis is generally deeper than it may at first appear, excision should be the treatment of choice. Vaporization of adhesions on the ovarian surface, bladder flap, and uterine peritoneum may be beneficial.
Uterosacral nerve ablation (LUNA) Since sensory nerves from the uterus run inside the uterosacral ligament, sometimes we will sever the ligament to relieve the pain associated with endometriosis.
This procedure relieves discomfort related in menstrual cramps in up to 85% of patients. Unfortunately LUNA does not relieve pain associated with adhesions, endometriomas and pelvic sidewall endometriosis.
Treatment of ovarian endometriomas has included removal of the ovary, simple drainage, destruction of the cyst-lining with laser, bipolar electrosurgery, monopolar electrosurgery, and excision of the ovarian cyst.
Although in many cases the cystlining can be stripped from inside the ovary during laparoscopy, in approximately 30% of the cases, this cannot be performed. In these cases, unless destruction of the lining is carried out, the endometrioma will likely recur. Use of an Argon beam coagulator, C02 laser or bipolar electrocautery are the methods of choice in this situation. Monopolar cautery must be used with caution as deeper penetration with this method may destroy normal ovarian tissue and cause premature ovarian failure.
Success Rate with Surgery
Pregnancy rates following surgery generally range between 35-40% for severe endometriosis to 55-65% with milder disease. Of those who become pregnant, 30 percent conceive within three months, 50 percent within six months, and 86 percent within fifteen months. Usually, normal monthly pregnancy rates can be achieved with ovulation induction and intrauterine insemination. Postoperative pregnancy rates appear best for those with infertility of short duration of one to two years of 68%. Those who have been trying between three and seven years have a 43% pregnancy rate, while those with eight or more years of infertility demonstrate a pregnancy rate of less than 10%.
When Hysterectomy May Be Appropriate
Complete hysterectomy-including removal of the ovaries-is the treatment of choice for women past their reproductive age. With this procedure the recurrence rate is only 1 to 3 percent. However, the use of estrogen-only hormone replacement or leaving an ovary behind significantly increase your risk that pain will recur. Up to 30% or more will experience recurrent endometriosis symptoms if both ovaries are not removed. For this reason I often recommend a hormone-free period before initiating hormone replacement therapy with a combination of estrogen and progesterone.

